

Roimata Smith shifts uncomfortably in her seat at the dining room table as she remembers some of the comments doctors have made to her over the last 57 years of her life. She wears a grey fleece-lined zip-up hoodie that she fidgets with. One upsetting memory, in particular, is repeatedly replaying in her head.
After moving to Auckland from Huntly to care for a whānau member this year, Roimata needed a new doctor. This was crucial for her as she has type 2 diabetes. She was running low on metformin, a standard diabetes drug that helps keep her blood sugar at a safe level, and needed a new prescription. But instead of walking out of the doctor’s office with a piece of paper to give to the pharmacist, she left feeling appalled and shocked.
"He didn’t check me for anything, blood pressure, he didn’t do any of that. He just walked in the room and said to me: ‘you’re fat’."
While in that small sterile room, she was also told by the doctor she needed to "go and get a job".
"He didn’t care how I felt, or anything about me. He just wanted to put someone down and he did a good job that day."

"I thought it was a joke. I didn’t think I really had it …. I didn’t really know the symptoms of diabetes."
Her 35-year-old daughter also has type 2 diabetes, but Roimata knew nothing about what it meant for her. When she got the news, she says she was offered little information about what to do.
"He said: ‘just try and change your diet’ and I thought ‘I’m not even on a diet’."
Her experience accessing healthcare has not been a good one. She distrusts the system that she says isn’t made for her. Unfortunately, people with experiences like Roimata are not hard to find.
An RNZ investigation into Māori healthcare, published this week, highlights diabetes as one of the biggest challenges.
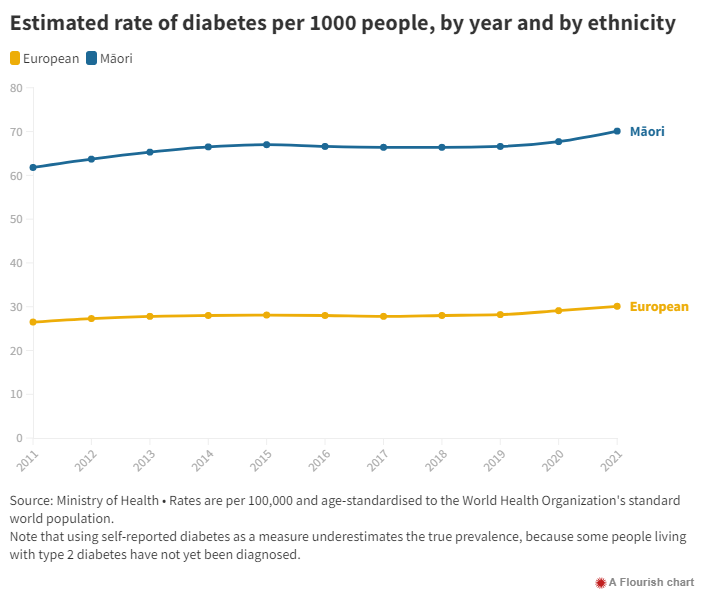
Diabetes is the country’s biggest and fastest-growing health condition. Ministry of Health figures show that in 2021 there were 302,778 people with diabetes, predominantly type 2. It occurs as a result of the body not producing enough insulin to maintain normal blood glucose (sugar) levels. While everyone needs some glucose in their blood, a high glucose level over time can harm your body.
The inequities for Māori are stark. According to the Ministry of Health, Māori are about twice as likely to have type 2 diabetes compared to non-Māori. Among people with diabetes, Māori are 2.8 times more likely than non-Māori to have renal failure, one of the complications of diabetes. Additionally, data obtained by RNZ under the Official Information Act show that Māori with diabetes are 1.5 times more likely than Europeans to have a diabetic limb amputation.
A PwC commissioned report released last year predicted that things could get a lot worse. It predicts the number of people with type 2 diabetes could rise by as much as 90 per cent across the next two decades to 430,000.
What makes such predictions even more frightening is a trend for younger people being diagnosed.
"In our Māngere clinic, type 2 diabetes is very common," says Dr Lily Fraser, the clinical director at Turuki Health in Māngere. Frazer specialises in diabetes care for Māori.
"What I’m seeing is that each generation of whānau that have diabetes, the next generation are getting it at least 10-20 years younger than the generation previous.
"For example, if your grandparents got diabetes, maybe in their 60s or 70s, then their children might get it in their 40s or 50s, and then what we’re seeing is their children are getting it in their 20s or 30s. And we have teenagers as well [with diabetes]….
"We are seeing multigenerational whānau with type 2 diabetes. We are worried about this and I’m really worried about 20-year-olds being put on long-term medication without other support being put in place to actually help them manage their diabetes in the long term."
Research published in 2018 showed that there were increasing numbers of children and teens under 15 in Auckland developing type 2 diabetes. It showed that Māori and Pacific children in New Zealand are up to 18 times more likely to develop type 2 diabetes than European children. The findings were based on 21 years of patient records from Starship’s paediatric diabetes service.

Type 2 diabetes can be inherited and connected to genetics and family history, although environmental variables also play a part. You’re more likely to get type 2 diabetes if a parent or sibling has it, but not everyone with a family history of the condition will.
When King received his diabetes diagnosis in 1990, he thought about his children.
"I felt a little bit depressed and you think, ‘oh my god, how’s this gonna affect the rest of my life?’ Especially because my daughter was only seven and my son was only five. So you think about the outlook for them because of what happened to my dad and what happened to his mum."
Amputations and dialysis treatment
Type 2 diabetes takes years off the life expectation for Māori. Not just that but it can also drastically reduce quality of life. When not managed well, it can lead to devastating health conditions and complications: sight loss, heart attacks, heart failure, kidney failure, strokes, and limb amputations.
Dr Brandon Orr-Walker is an endocrinologist and diabetes specialist at Middlemore Hospital in South Auckland, the region most affected by diabetes. Last year, there were 51,268 people with diabetes in Counties Manukau alone, roughly the same size as the population of Nelson. Middlemore Hospital is also home to the largest dialysis service in Australasia.

"Self management and access to care, a reluctance to manage things, a case of prioritisation. That comes down to security of food and home and shelter, and so forth. Today’s struggles may prevent people from looking forward to tomorrow’s health. It’s a whole range of things.
"I think that one of the problems we’ve gained in the past is a narrative where people have talked about self-responsibility or have talked about environmental problems without really taking on board the fact that it’s actually all of these things. It’s much more complicated than just attributing it to one thing."
But he also explains that, unfortunately for Māori, they are genetically more at risk from the consequences of type 2 diabetes. He uses the analogy of sunburn when explaining how it works to patients.
"I say: Look, you and I need to be careful if we go out into the sun on a summer’s day, because we will get burned. But as a Pākehā with fairer skin, rather than saying, ‘oh, well, that’s just the way it is’ and being fatalistic, I need to be extra protective because of having paler skin.
"Now, the same sort of susceptibility by analogy is present for Māori in particular for kidney disease, but also for other fine blood vessel problems. And so there is a greater reason to be well protected, and that’s clearly genetic."
Orr-Walker is right, Māori are 2.8 times more likely than non-Māori to have renal or kidney failure for which the leading cause is type 2 diabetes.
"I think the raw numbers of how many people [with diabetes] are only part of the story, the real issue is how well the diabetes is controlled and the complications of diabetes.
"The mass effect of this and the deep scars it’s already creating in terms of the health of individuals, communities, the health of whānau by its size alone has to be number one," he says.
Graham King watched his late father get hooked up to a dialysis machine three days a week, for five hours each time, which he says took over his father’s whole life.
"It would be an all-day affair. My mother would drive him from Kawakawa Bay and drop him off. Then either me or one of my brothers would pick him up and drop him home. So that was a long process.
"He found it difficult being there."
King’s father also had four toes amputated, another complication of type 2 diabetes.
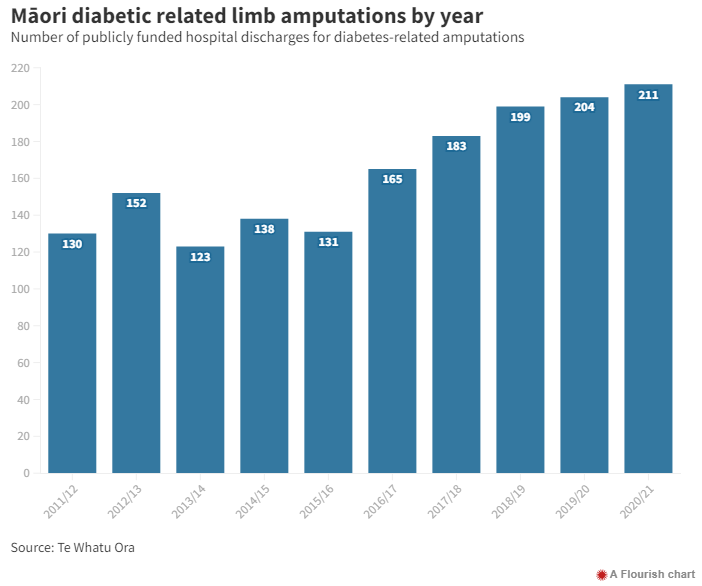
The 880 diabetic limb amputations done last year cost the country over $23m.
Orr-Walker says at the current rate, it’s only going to get worse. He stresses the urgency of the problem for Māori and Pasifika.
"For a long time we’ve said that type 2 diabetes is a tsunami. It is a disaster in slow motion. But unfortunately, the ‘slow motion-ness’ of it means that it’s just a little easy to forget about and not act with sufficient urgency."
How did it get this bad? Well, racism.
Selah Hart is the chief executive of Hāpai te Hauora, an Auckland-based organisation that advocates for Māori public health outcomes. She says the current statistics show that the health system has continued to fail Māori and those in lower socioeconomic brackets.
"The writing’s clear as day on the wall that the system has been fragmented, it is what many are referring to as a postcode lottery. But I think we could go even deeper into that. It isn’t just the postcode lottery, it isn’t just based on where your residential address is, it’s actually also based on the ethnic group that you belong to, because we know that there are inherent biases in the system."
A University of Waikato study published in 2020 found that Māori patients receive fewer prescriptions of metformin, a common diabetes drug, than non-Māori patients and have worse blood sugar control as a result. It showed that while Māori received fewer prescriptions than non-Māori, there was no difference in adhering to prescriptions, likely due to access to prescriptions rather than the medication dispensing.
This study backs up a 2018 Pharmac-commissioned University of Auckland report which showed that in 2012/13, Māori received pharmaceutical treatments at a rate 41% below what non-Māori would when presenting with the same health needs. The drivers of such inequities, it said, were "complex and entrenched" - the result of historical and contemporary social, political, cultural and economic processes. A "deeper understanding of systems and barriers" was needed to overcome medicine inequities. In the Māori health sector, this is known as the ‘mission million.’
While neither study addressed the reasons for fewer prescriptions in detail, Dr Lily Frazer says it’s unconscious bias from doctors. She says doctors must consider their assumptions when treating each patient.
"Have I already decided for this person just based on their ethnicity or based on their name or based on their address that they’re not going to take it and so I’m not even going to offer it? That definitely happens in health, from GPs from, all medical professionals, really."
When Roimata Smith recalls the day the doctor called her fat and didn’t prescribe her diabetes medication, she says she knows why he treated her the way he did.
"It’s the colour of my skin … but then they shouldn’t be looking at the colour of your skin."
Good kai, bad kai
Over the last 200 years, Māori eating habits have undergone a significant transformation. Pre-colonisation, research shows that the traditional diet for Māori was typically low in carbs and consisted of meat, vegetables, and seafood that were either hunted or harvested. Wheat, potatoes, maize, and other vegetables were introduced by Pākehā settlers and quickly embraced by Māori. Since the US implemented low-fat, high-carbohydrate dietary recommendations in the 1970s, there has been an enormous rise in obesity and the comorbidities that go along with it globally.
Since 2015, Frazer’s clinic has been recommending a low-carb, ketogenic fasting diet to treat type 2 diabetes patients, which she sees as similar to how her tīpuna (ancestors) ate. She says it’s not fat causing insulin resistance; it’s carbohydrates and sugars.
"I don’t think our tīpuna were getting up and having a big breakfast or a breakfast, morning tea, lunch, afternoon tea, and dinner. … and obviously, our kai was unprocessed, whole foods and the healthy fats that come with the bird or come with the fish.
"It’s capturing the lessons of that style of eating and being more in tune with the environment."
Even over her lifetime, she says the way people eat and drink has changed significantly, impacting the rise in type 2 diabetes.
"The access to sugary drinks, lollies not being just for a party, but just being a food, frequent takeaways, all those things have an impact."
She is hopeful that the new health system will recognise the role this way of eating plays in managing type 2 diabetes.
"I’m hopeful that in this revamp of the health system, that somewhere in there somebody is really looking seriously at the kai that we recommend for whānau who have type 2 diabetes."
But Hamilton-based Māori nurse, Hinemanu Kelly, says the patients she sees can’t afford healthy foods.
"All the time when I talk to people about making some changes to their menu, there are a good amount of them that will say ‘oh we can’t get fruit or veggies because they are too expensive’. Because at the end of the day they go and buy what is on special and right now fruit and veggies are just so expensive so it’s definitely not a priority for our unwell whānau to be buying stuff they can’t afford."
Roimata Smith is currently on the job seekers’ benefit. After emergency housing payment deductions and other medical bills, she only has $150 each week to live on.
She budgets $30-$50 for food each week, which, with the current cost of living crisis, doesn’t go far, however hard she tries.
"I can’t afford veggies, meat. If I can’t afford it, I don’t buy it. I just stick with canned food … not that I like it."
Opening a can of spaghetti or baked beans is a typical dinner for her.
Whakawhanaungatanga
To help the lifestyle change needed to manage type 2 diabetes, Turuki Health in Māngere employs health coaches.
"Lifestyle change is a journey, and It’s not going to happen over a 15 minute consultation with a GP, because you just don’t have the time, or the accessibility to the doctor to be able to make those sustainable changes." says Frazer.
She believes their care method is working for Māori. It’s a system based on whakawhanaungatanga, establishing and building relationships with the people she cares for.
"We always say that relationships are at the heart of successful change and so that’s something we do focus on for everybody at Turiki."
Frazer also stresses that when whānau are diagnosed with type 2 diabetes, they should not be made to feel it is their fault.

"You have to say, ‘what’s going on for you that is making this a problem?’ Is it a) that you don’t have enough understanding around this that you haven’t been getting enough support to understand your diagnosis? Is it b) you don’t actually have the money to eat healthily and have a diabetes right diet? Or is it c) that you’ve actually had a really difficult experience with a health practitioner, and now you don’t have any trust in that system."
She says it’s usually all of the above.
‘There’s no quick fix to cure diabetes’
In October this year, Te Whatu Ora and Te Aka Whai Ora (Health NZ and the Māori Health Authority) released Te Pae Tata, the interim New Zealand Health Plan, which sets out the priorities for the next two years and replaces 20 different district annual plans from the old district health boards.
The plan has six key priorities, one of which is Māuiuitanga taumaha - people living with chronic health conditions, which includes diabetes.
Chief executive of Te Aka Whai Ora, Riana Manuel, has some big aspirations when it comes to improving chronic conditions among Māori. But there’s a catch - she says it will take time.
"You can’t just look at this problem and go: ‘Oh it’s a one-dimensional fix, we just need to apply more medication, or we need to have more access to GP services.’ Actually, we need lifestyle changes. Chronic disease is about the big, gnarly, transformative things that take time. They’re not often popular things. There’s no quick fix to cure diabetes," Manuel says.
"We know that we can make a huge impact in chronic conditions, when our people are living in better housing, when they have better economic basis, that then allows them to buy good kai that is going to be better for them … but that takes time."
She says the way they will do that is to drive better health literacy for Māori, better access to a range of services, increased screening for chronic conditions and improvement on social determinants, like housing and poverty.
"Poverty will always drive poor health outcomes. That’s just a fact. If you cannot afford the things you need to live the kind of life that you need to lead, then that’s going to be problematic."
How will Te Aka Whai Ora improve social determinants?
"By working together across the sectors to make sure that we can actually implement things that are going to be really meaningful to turn that around."
The interim health plan says it will also "implement accessible and nationally-consistent clinical pathways for diabetes, cardiovascular diseases, respiratory conditions, stroke and gout, supporting specialist teams to integrate with primary and community care providers to create seamless pathways for whānau."
Back in Roimata Smith’s living room, she is just starting to regain trust in the healthcare system after the shocking incident where a doctor called her fat.
These days, she has a new GP, a Māori woman, and a Māori mobile nurse who comes and visits her in her whare.
As for the racist doctor she met, she says she hopes he’s the last one that she comes across.
"I don’t want to go through that with any other doctor like that. I wouldn’t expect anyone else would want to either."
- Ella Stewart, RNZ











